

No, not a pit stop. A Pit Break! It is a term you may hear in the delivery room at the hospital during a medical induction.

But what is a Pit Break, when should you ask for one and how can you use it to your advantage?
If you are induced or need labor augmentation, Pitocin is commonly administered intravenously (through an IV). Pitocin is a synthetic version of the naturally occurring hormone oxytocin. Some birth workers in the hospital will call Pitocin oxytocin however, they are not the same thing.
Oxytocin also known as the "love hormone" is one of the major hormones at play in labor causing contractions as well as progressing said contractions. It is the main driver or orchestrator in the labor process directing the symphony of hormones that work on a feedback loop ultimately leading to birth in a physiological birth setting. Oxytocin is produced in high amounts at the end of pregnancy and also when we feel safe, secure, comfortable and are in a parasympathetic or "rest and digest" nervous system state.
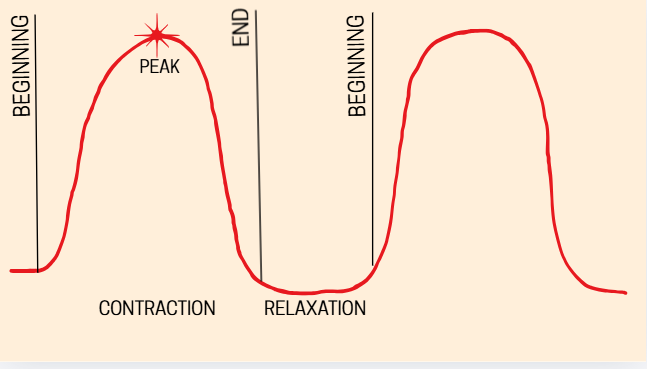
Pitocin is a synthetic uterine stimulant working primarily to contract the uterus. The contractions caused by Pitocin are not the same as natural contractions, so Pitocin does not entirely replicate oxytocin. In many cases Pitocin causes unnaturally strong, intense, non-stop contractions that are very close together. Contractions that occur naturally by the presence of Oxytocin on the other hand are wave like. A woman experiencing physiological or natural labor can feel them starting to come on and they will slowly build in intensity, peaking at about halfway through and then decreasing in intensity to a full rest in between. You will also see natural progression during labor with them starting further apart and not very intense, slowly increasing in intensity and frequency. See the image below for a greater understanding of a natural contraction and their wave like pattern. This natural contraction pattern is what we typically see in labor that has not been induced using Pitocin or other methods.
In addition to the Pitocin induced contractions being much more intense they are also not accompanied by the rise in hormones that promote natural pain relief like beta-endorphins. During natural labor as Oxytocin rises not only is the pain gradually increasing in intensity, but our body also has a wonderful mechanism to counter act the pain known as beta- endorphins. Similar hormones are released for runners after a long, hard race- think a "runners high." This hormone is known to be 18-33 times more effective at pain management than morphine! Pitocin however doesn't cross the brain barrier, so the same hormone loop is not created resulting in strong contractions with no natural relief.
While Pitocin can be a great tool to use to induce and potentially facilitate vaginal birth when other circumstances may be making it otherwise difficult or impossible, we have seen that the rate at which it is used is rising and, in most cases, not necessary. We now also have new research showing that the Cascade of intervention is a reality. This essentially means that the use of Pitocin does lead to the increased chance of having a C-section, which once was simply anecdotal is now confirmed by research. The C-section rates are now at an all-time high in America, at 31% of all births, whereas the WHO recommends it being at no more than 10%. Any rate higher than 10% is shown to have no impact on the health and wellness of mother or baby. How can we reduce this percentage for more optimal birth outcomes?
Often in labor where Pitocin is used and contractions become too difficult for the birthing woman to manage; an Epidural is often jumped to for pain relief and rest. Something that is not talked about enough that can help this type of labor be more manageable and ultimately lead to more vaginal births is a Pitocin Break. This intervention may be a good first step instead of jumping right for an Epidural because there are no adverse effects that could inhibit natural birth whereas with an epidural there are. More on the Epidural here! A Pitocin Break can potentially help a woman get the benefits needed from Pitocin without the unnecessary cascade of other medical interventions.
Enter Pit Break
A Pitocin Break also known as a Pit break is the discontinuation of Pitocin when necessary, during labor. How come this isn't more commonly talked about being that labor augmented by Pitocin is known to be intense and known to increase the chance of C-section?
When labor is induced using Pitocin in most cases it is because the Healthcare group the woman is under put her on a timeline. One of the following is probably true:
- She is overdue (Depends on your providers policy. Don't want to be on a clock, check out this blog.)
- Labor is taking too long
- PROM (premature rupture of membranes) or the breaking of waters before contractions begin. Hospitals usually give women no more than 24 hours to be in active labor after their water breaks before induction
- There is a medical need to get labor going i.e. Preeclampsia, High Blood Pressure, Restricted Fetal Growth
However, did you know Pitocin is not the only way to induce labor? More on this topic here!
When a woman is put under pressure to have the baby at a certain time it can and in most cases will stress her out, this stress then shuts down her natural labor progression increasing the need then for more Pitocin. In the scenarios mentioned above there is so much nuance and it's important to know for yourself how much of a risk there actually is and why there may be an increased need for induction or not. These are important conversations to have when choosing a healthcare provider or midwife to care for you and your growing family.
Doctors will want to slowly increase the amount of Pitocin she is given overtime. Starting at about 0.5-2 milliunits per minute depending on hospital policy up to 20 milliunits. This is shown to cause stronger contractions and progress labor. The amount of Pitocin used varies from woman to woman, the birth team is looking for when contractions are most effective. However, with the increase the contractions may become more and more unbearable. Once the woman can no longer manage the pain an Epidural is typically recommended. This continues what is known as the Cascade of Intervention. Check out this video on the Cascade of Intervention!
There is an alternate route one can take. A Pit Break. If you can no longer manage the contractions, are feeling you need to rest, or even if you want to see if your body will continue to labor on its own you can request a break from the Pitocin. The half-life of Pitocin is very short, meaning in about 1-2 hours it should all be cleared from your body.
In some cases, the birth team will actually suggest taking a Pit break. This occurs when they feel:
- The contractions are too intense and/or ineffective
- Uterine Hyperstimulation
- Augmented labor lasts more than 12-18 hours
- Oxytocin receptor desensitization is suspected
A break should be taken ideally for 4-8 hours to allow for optimal rest of the uterus. Evidence shows that Pitocin may even be more effective and reduce fetal distress when breaks are given. If a woman has a higher risk of uterine rupture like attempting a VBAC, breaks should be taken more frequently.
A 2015 study shows us that taking a Pit break once the woman is in active labor results in shorter labor time as well as less Pitocin used. This can then make labor less expensive and also reduce the risks associated with the use of higher doses of Pitocin. There is also a recent meta-analysis showing that Pitocin discontinuation in active labor reduces the likelihood of C-section by 20%.
Conclusion

In conclusion it's important to first and foremost remember there is no one size fits all for anything, but, in this case particularly, labor and birth outcomes are on a case-by-case basis. Pitocin induction as well as the specifics of taking a Pit break depends entirely on individual circumstances.
My intention when writing this blog was to simply inform you that this option exists and why it may be beneficial to consider during your labor and birth process. It can potentially help to avoid the continuation of medical intervention past the use of this medication as well as help to avoid an emergency C-section or one that is not medically necessary. Ultimately resulting in more positive and less traumatic birth outcomes!
Add comment
Comments